Biomechanical properties of AAA – what does it mean to clinicians who are faced with dilemma - To do or not to do an intervention based on the size of the AAA?
Abdominal aortic aneurysms are feared in the clinical practice as they are known to rupture without a prior notice and result in death. This clinical fear of rupture supports the treatment of the large aneurysms even though they are asymptomatic. But, open operative repair of the small AAA is associated with significant risks which are more in units which are not considered large volume centers. That means we have to be more selective in identifying the AAAs which are likely to rupture based on their wall ability to withstand the stress and strain. The bio mechanical properties of the normal aortic wall and aneurysm wall are definitely going to help us in selecting the patients for early repair in addition to the diameter.
In the year 1966 Szilagyi et al observed that the aneurysms larger than 6 cm are at increased risk of rupture. Later Foster and colleagues noted similar observations (< 6cm – 16% ., >6cm 51% rupture). For the next 4 decades the diameter of the aneurysm dictated the decision to operate. Now we are looking at the other parameters such as “wall stress”.
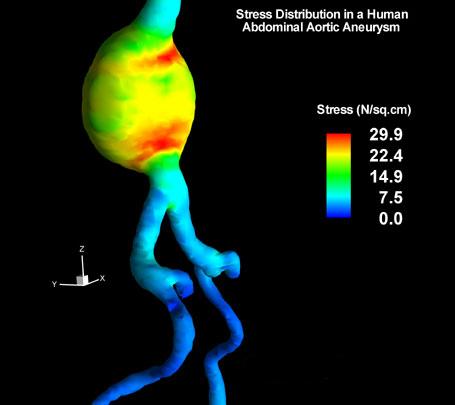
Finite Element analysis (2002) was introduced by Fillinger colleagues was used to assess the wall stress in the aortic aneurysms (see fig). The figure shows stress as Newtons/ cm2. The point of maximum stress need not be over the maximum diameter point. There are many factors in wall structure which could be deciding the strength of the wall to resist the breakdown. Finite element analysis method was used by engineers to study the elastic properties and strength the materials. The same is applied to the biological materials where the shapes are variable such as the aortic dilatation. In women the aneuryms with small diameters are also risk of rupture (5cm). The measurement of wall stress with finite element analysis is not universally accepted and validated as a method for assessing risk of rupture. But in the coming years it may be available in our neighborhood and we may assess the aneurysms with this method to predict rupture. This is comparable to the foot pressures (pedobarograph) to assess the development of plantar foot ulcers. Probably we will be able to get this information along with CT scan report and imagine the ease with which the surgeon can tell his patients about the need for interventions.